
BEIJING & CAMBRIDGE, Mass.--(BUSINESS WIRE)--$BGNE #BTKi--BeiGene, Ltd. (NASDAQ: BGNE; HKEX: 06160), a global biotechnology company focused on developing and commercializing innovative medicines worldwide, today announced that the China National Medical Products Administration (NMPA) has conditionally approved KYPROLISďż˝ (carfilzomib) for injection in combination with dexamethasone for the treatment of adult patients with relapsed or refractory (R/R) multiple myeloma who have received at least two prior therapies, including a proteasome inhibitor and an immunomodulatory agent. KYPROLIS is licensed to BeiGene in China under a strategic collaboration with Amgen. This is the first approval for KYPROLIS in China.

�Multiple myeloma is an incurable and highly recurrent hematological malignancy. Unfortunately, the clinical needs of patients in China with this disease have yet to be fully satisfied,� commented Xiaobin Wu, Ph.D., President, Chief Operating Officer, and General Manager of China at BeiGene. �The approval of KYPROLIS provides us with an important opportunity to offer adult patients in China with relapsed or refractory multiple myeloma a proteasome inhibitor with high selectivity and irreversibility as a treatment option for their disease. With a commercial organization of more than 2,200 people in China we are excited to add KYPROLIS to our product portfolio, which now includes eight approved cancer treatments.�
The conditional approval of KYPROLIS was based on results from the Phase 3 trial (NCT03029234) in China evaluating the efficacy and safety of KYPROLISplus dexamethasone in 123 patients with R/R multiple myeloma. Results of the trial showed that the efficacy in Chinese patients who had received a median of four prior lines of therapy were generally consistent with that seen in the global studies. The overall response rate, the primary endpoint, was 35.8% (95% CI: 27.3, 44.9). The median progression-free survival (PFS) assessed by Independent Review Committee (IRC) was 5.6 months (95% CI: 4.6, 6.5). The safety profile observed for Chinese patients in this study was consistent with that observed in the global studies evaluating KYPROLIS in R/R multiple myeloma. In global studies, the most common adverse reactions in the combination therapy trials were anemia, diarrhea, fatigue, hypertension, pyrexia, upper respiratory tract infection, thrombocytopenia, cough, dyspnea, and insomnia. No new safety risks were identified based on analyses of adverse events in Chinese patients. Full approval is subject to results of a confirmatory trial.
About Multiple Myeloma
Multiple myeloma (MM) is a cancer of the white blood cell, which accumulates in bone marrow and interrupts normal cell function and processes1. It is the second most common hematologic malignancy, accounting for ~1% of all cancers and 13% of hematologic cancers2,3,4. MM is often diagnosed in later stages and nearly 20% of patients may experience disease reoccurrence or relapse after initial treatment5,6. It is estimated that there were 16,500 new cases and 10,300 deaths due to MM in China during 2016, with a higher prevalence in males and older adults ages 55 and 74 years old6,7,8. Uncontrolled MM leads to complications including pathologic fractures and anemia.
About KYPROLISďż˝ (carfilzomib) for injection
Proteasomes play an important role in cell function and growth by breaking down proteins that are damaged or no longer needed. KYPROLIS has been shown to block proteasomes, leading to an excessive build-up of proteins within cells. In some cells, KYPROLIS can cause cell death, especially in myeloma cells because they are more likely to contain a higher amount of abnormal proteins.
Since its first approval in 2012, approximately 150,000 patients worldwide have received KYPROLIS. KYPROLIS is approved in the U.S. for the following:
-
for the treatment of adult patients with relapsed or refractory multiple myeloma who have received one to three lines of therapy in combination with
- Lenalidomide and dexamethasone; or
- Dexamethasone; or
- Daratumumab and dexamethasone.
- as a single agent for the treatment of adult patients with relapsed or refractory multiple myeloma who have received one or more lines of therapy.
KYPROLIS is also approved in countries or regions including Algeria, Argentina, Australia, Bahrain, Belarus, Brazil, Canada, Chile, Colombia, Ecuador, Egypt, European Union, Hong Kong, India, Israel, Japan, Jordan, Kazakhstan, Kuwait, Lebanon, Macao, Malaysia, Mexico, Morocco, New Zealand, Oman, Peru, Philippines, Qatar, Russia, Saudi Arabia, Serbia, Singapore, S. Africa, S. Korea, Switzerland, Taiwan, Thailand, Turkey and United Arab Emirates.
Important U.S. Safety Information
U.S. INDICATIONS
- KYPROLISďż˝ (carfilzomib) is indicated in combination with dexamethasone or with lenalidomide plus dexamethasone or with daratumumab and dexamethasone for the treatment of adult patients with relapsed or refractory multiple myeloma who have received one to three lines of therapy.
- KYPROLISďż˝ is indicated as a single agent for the treatment of adult patients with relapsed or refractory multiple myeloma who have received one or more lines of therapy.
IMPORTANT U.S. SAFETY INFORMATION FOR KYPROLIS
Cardiac Toxicities
- New onset or worsening of pre-existing cardiac failure (e.g., congestive heart failure, pulmonary edema, decreased ejection fraction), cardiomyopathy, myocardial ischemia, and myocardial infarction including fatalities have occurred following administration of KYPROLIS. Some events occurred in patients with normal baseline ventricular function. Death due to cardiac arrest has occurred within one day of administration.
- Monitor patients for signs or symptoms of cardiac failure or ischemia. Evaluate promptly if cardiac toxicity is suspected. Withhold KYPROLIS for Grade 3 or 4 cardiac adverse reactions until recovery, and consider whether to restart at 1 dose level reduction based on a benefit/risk assessment.
- While adequate hydration is required prior to each dose in Cycle 1, monitor all patients for evidence of volume overload, especially patients at risk for cardiac failure. Adjust total fluid intake as clinically appropriate.
- For patients ? 75 years, the risk of cardiac failure is increased. Patients with New York Heart Association Class III and IV heart failure, recent myocardial infarction, conduction abnormalities, angina, or arrhythmias may be at greater risk for cardiac complications and should have a comprehensive medical assessment prior to starting treatment with KYPROLIS and remain under close follow-up with fluid management.
Acute Renal Failure
ďż˝ Cases of acute renal failure, including some fatal renal failure events, and renal insufficiency (including renal failure) have occurred. Acute renal failure was reported more frequently in patients with advanced relapsed and refractory multiple myeloma who received KYPROLIS monotherapy. Monitor renal function with regular measurement of the serum creatinine and/or estimated creatinine clearance. Reduce or withhold dose as appropriate.
Tumor Lysis Syndrome
- Cases of Tumor Lysis Syndrome (TLS), including fatal outcomes, have occurred. Patients with a high tumor burden should be considered at greater risk for TLS. Adequate hydration is required prior to each dose in Cycle 1, and in subsequent cycles as needed. Consider uric acid lowering drugs in patients at risk for TLS. Monitor for evidence of TLS during treatment and manage promptly, and withhold until resolved.
Pulmonary Toxicity
- Acute Respiratory Distress Syndrome (ARDS), acute respiratory failure, and acute diffuse infiltrative pulmonary disease such as pneumonitis and interstitial lung disease have occurred. Some events have been fatal. In the event of drug?induced pulmonary toxicity, discontinue KYPROLIS.
Pulmonary Hypertension
- Pulmonary arterial hypertension (PAH) was reported. Evaluate with cardiac imaging and/or other tests as indicated. Withhold KYPROLIS for PAH until resolved or returned to baseline and consider whether to restart based on a benefit/risk assessment.
Dyspnea
- Dyspnea was reported in patients treated with KYPROLIS. Evaluate dyspnea to exclude cardiopulmonary conditions including cardiac failure and pulmonary syndromes. Stop KYPROLIS for Grade 3 or 4 dyspnea until resolved or returned to baseline. Consider whether to restart based on a benefit/risk assessment.
Hypertension
- Hypertension, including hypertensive crisis and hypertensive emergency, has been observed, some fatal. Control hypertension prior to starting KYPROLIS. Monitor blood pressure regularly in all patients. If hypertension cannot be adequately controlled, withhold KYPROLIS and evaluate. Consider whether to restart based on a benefit/risk assessment.
Venous Thrombosis
- Venous thromboembolic events (including deep venous thrombosis and pulmonary embolism) have been observed. Provide thromboprophylaxis for patients being treated with the combination of KYPROLIS with dexamethasone or with lenalidomide plus dexamethasone or with daratumumab and dexamethasone. The thromboprophylaxis regimen should be based on an assessment of the patient�s underlying risks.
- For patients using hormonal contraception associated with a risk of thrombosis, consider an alternative method of effective contraception during treatment.
Infusion-Related Reactions
- Infusion-related reactions, including life?threatening reactions, have occurred. Signs and symptoms include fever, chills, arthralgia, myalgia, facial flushing, facial edema, laryngeal edema, vomiting, weakness, shortness of breath, hypotension, syncope, chest tightness, or angina. These reactions can occur immediately following or up to 24 hours after administration. Premedicate with dexamethasone to reduce the incidence and severity of infusion-related reactions.
Hemorrhage
- Fatal or serious cases of hemorrhage have been reported. Hemorrhagic events have included gastrointestinal, pulmonary, and intracranial hemorrhage and epistaxis. Promptly evaluate signs and symptoms of blood loss. Reduce or withhold dose as appropriate.
Thrombocytopenia
- KYPROLIS causes thrombocytopenia with recovery to baseline platelet count usually by the start of the next cycle. Monitor platelet counts frequently during treatment. Reduce or withhold dose as appropriate.
Hepatic Toxicity and Hepatic Failure
- Cases of hepatic failure, including fatal cases, have occurred. KYPROLIS can cause increased serum transaminases. Monitor liver enzymes regularly regardless of baseline values. Reduce or withhold dose as appropriate.
Thrombotic Microangiopathy
- Cases of thrombotic microangiopathy, including thrombotic thrombocytopenic purpura/hemolytic uremic syndrome (TTP/HUS), including fatal outcome, have occurred. Monitor for signs and symptoms of TTP/HUS. Discontinue if diagnosis is suspected. If the diagnosis of TTP/HUS is excluded, KYPROLIS may be restarted. The safety of reinitiating KYPROLIS is not known.
Posterior Reversible Encephalopathy Syndrome (PRES)
- Cases of PRES have occurred in patients receiving KYPROLIS. If PRES is suspected, discontinue and evaluate with appropriate imaging. The safety of reinitiating KYPROLIS is not known.
Progressive Multifocal Leukoencephalopathy (PML)
- Cases of PML, including fatal cases, have occurred. In addition to KYPROLIS, other contributary factors may include prior or concurrent use of immunosuppressive therapy. Consider PML in any patient with new onset of or changes in pre-existing neurological signs or symptoms. If PML is suspected, discontinue and initiate evaluation for PML including neurology consultation.
Increased Fatal and Serious Toxicities in Combination with Melphalan and Prednisone in Newly Diagnosed Transplant-ineligible Patients
- In a clinical trial of transplant-ineligible patients with newly diagnosed multiple myeloma comparing KYPROLIS, melphalan, and prednisone (KMP) vs bortezomib, melphalan, and prednisone (VMP), a higher incidence of serious and fatal adverse reactions was observed in patients in the KMP arm. KMP is not indicated for transplant-ineligible patients with newly diagnosed multiple myeloma.
Embryo-fetal Toxicity
- KYPROLIS can cause fetal harm when administered to a pregnant woman.
- Advise pregnant women of the potential risk to a fetus. Females of reproductive potential should use effective contraception during treatment with KYPROLIS and for 6 months following the final dose. Males of reproductive potential should use effective contraception during treatment with KYPROLIS and for 3 months following the final dose.
Adverse Reactions
- The most common adverse reactions in the combination therapy trials: anemia, diarrhea, fatigue, hypertension, pyrexia, upper respiratory tract infection, thrombocytopenia, cough, dyspnea, and insomnia.
- The most common adverse reactions in monotherapy trials: anemia, fatigue, thrombocytopenia, nausea, pyrexia, dyspnea, diarrhea, headache, cough, edema peripheral.
Please see accompanying full Prescribing Information.
BeiGene Oncology
BeiGene is committed to advancing best and first-in-class clinical candidates internally or with like-minded partners to develop impactful and affordable medicines to patients across the globe. We have a growing R&D team of approximately 2,300 colleagues dedicated to advancing more than 90 clinical trials involving more than 13,000 patients. Our expansive portfolio is directed by a predominantly internalized clinical development team supporting trials in more than 40 countries or regions. Hematology-oncology and solid tumor targeted therapies and immuno-oncology are key focus areas for the Company, with both mono- and combination therapies prioritized in our research and development. The Company currently markets three medicines discovered and developed in our labs: BTK inhibitor BRUKINSA in the United States, China, Canada, and additional international markets; and non-FC-gamma receptor binding anti-PD-1 antibody tislelizumab and PARP inhibitor pamiparib in China.
BeiGene also partners with innovative companies who share our goal of developing therapies to address global health needs. We commercialize a range of oncology medicines in China licensed from Amgen and Bristol Myers Squibb. We also plan to address greater areas of unmet need globally through our collaborations including with Amgen, Bio-Thera, EUSA Pharma, Mirati Therapeutics, Seagen, and Zymeworks. BeiGene has also entered into a collaboration with Novartis granting Novartis rights to develop, manufacture, and commercialize tislelizumab in North America, Europe, and Japan.
About BeiGene
BeiGene is a global, science-driven biotechnology company focused on developing innovative and affordable medicines to improve treatment outcomes and access for patients worldwide. With a broad portfolio of more than 40 clinical candidates, we are committed to expediting the development of our diverse pipeline of novel therapeutics through collaborations or our own internal capabilities, with the aspirational goal of radically improving access to medicines for two billion more people by 2030. BeiGene is a headquarter-less company by design, with a growing global team of approximately 6,000 colleagues across five continents. To learn more about BeiGene, please visit www.beigene.com and follow us on Twitter at @BeiGeneGlobal.
Forward-Looking Statements
This press release contains forward-looking statements within the meaning of the Private Securities Litigation Reform Act of 1995 and other federal securities laws, including statements regarding the commercialization and potential benefits of KYPROLIS; BeiGene�s plans and expectations for the commercialization of its and Amgen�s other oncology products and pipeline assets; and BeiGene�s plans, commitments, aspirations and goals under the headings �BeiGene Oncology� and �About BeiGene�. Actual results may differ materially from those indicated in the forward-looking statements as a result of various important factors, including BeiGene's ability to demonstrate the efficacy and safety of its drug candidates; the clinical results for its drug candidates, which may not support further development or marketing approval; actions of regulatory agencies, which may affect the initiation, timing and progress of clinical trials and marketing approval; BeiGene's ability to achieve commercial success for its marketed products and drug candidates, if approved; BeiGene's ability to obtain and maintain protection of intellectual property for its technology and drugs; BeiGene's reliance on third parties to conduct drug development, manufacturing and other services; BeiGene�s limited operating history and BeiGene's ability to obtain additional funding for operations and to complete the development and commercialization of its drug candidates; the impact of the COVID-19 pandemic on the Company�s clinical development, commercial and other operations, as well as those risks more fully discussed in the section entitled �Risk Factors� in BeiGene�s most recent quarterly report on Form 10-Q, as well as discussions of potential risks, uncertainties, and other important factors in BeiGene's subsequent filings with the U.S. Securities and Exchange Commission. All information in this press release is as of the date of this press release, and BeiGene undertakes no duty to update such information unless required by law.
KYPROLISďż˝ is a registered trademark of Amgen Inc.
- https://www.mayoclinic.org/diseases-conditions/multiple-myeloma/symptoms-causes/syc-20353378#:~:text=Multiple%20myeloma%20is%20a%20cancer,crowd%20out%20healthy%20blood%20cells.
- Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. (2011) 364:1046�60. doi: 10.1056/NEJMra1011442.
- Raab MS, Podar K, Breitkreutz I, Richardson PG, Anderson KC. Multiple myeloma. Lancet. (2009) 374:324�39. doi: 10.1016/S0140-6736(09)60221-X.
- Kazandijan D. Multiple myeloma epidemiology and survival, a unique malignancy. Semin Oncol. 2016 Dec; 43(6): 676�681.
- Majithia N, Rajkumar SV, Lacy MQ, et al. Early relapse following initial therapy for multiple myeloma predicts poor outcomes in the era of novel agents. Leukemia. 2016;30(11):2208-2213. doi:10.1038/leu.2016.147.
- Li J, Wang Y, Liu P. The impact on early diagnosis and survival outcome of M-protein screening-driven diagnostic approach to multiple myeloma in China: a cohort study. J Cancer 2019; 10(20):4807-4813. doi:10.7150/jca.32103.
- Liu J, Liu W, Mi L, et al. Incidence and mortality of multiple myeloma in China, 2006-2016: an analysis of the Global Burden of Disease Study 2016. J Hematol Oncol. 2019;12(1):136. Published 2019 Dec 10. doi:10.1186/s13045-019-0807-5.
- Wang S, Xu L, Feng J, et al. Prevalence and Incidence of Multiple Myeloma in Urban Area in China: A National Population-Based Analysis. Front Oncol. 2020;9:1513. Published 2020 Jan 24. doi:10.3389/fonc.2019.01513.
Contacts
Investor Contact
Gabrielle Zhou
+86 10-5895-8058
[email protected]
Media Contact
Liza Heapes or Vivian Ni
+1 857-302-5663 or +1 857-302-7596
[email protected]
More from miscw.com
 TUMI’s TEGRA-LITE® Comes to Hyper-Realistic Life In a Groundbreaking New Campaign
TUMI’s TEGRA-LITE® Comes to Hyper-Realistic Life In a Groundbreaking New Campaign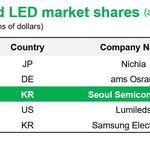 Seoul Semiconductor: Korea’s Optical Semiconductor Company, Reaffirms its Third Ranking in the Global Market
Seoul Semiconductor: Korea’s Optical Semiconductor Company, Reaffirms its Third Ranking in the Global Market Alive Drumming’s New Release of Song Rhythm Tracks
Alive Drumming’s New Release of Song Rhythm Tracks- Subtonomy Attends GITEX to Showcase How its Platform Helps Speed and Empower Telco Artificial Intelligence (AI) Initiatives





